More Than a Neck Problem: Unpacking the Mystery of Thoracic Outlet Syndrome
If you spend your days hunched over a keyboard, you are no stranger to neck pain. For millions of office workers and manual labourers, a stiff neck and the occasional “pins and needles” sensation in the hand are simply the price of admission to modern life. We usually chalk it up to poor posture, buy a new ergonomic chair, or assume we have a “pinched nerve” in the spine.
But for a surprising number of people, the symptoms tell a different story—one that has nothing to do with the vertebrae or discs at all.
This clinical picture is a powerful reminder that not all arm and neck pain originates in the spine. In fact, many cases of persistent upper limb pain are caused by a condition known as Vascular Thoracic Outlet Syndrome (TOS), a disorder that is often missed, frequently misdiagnosed, and requires a completely different treatment pathway than standard back or neck pain.
The Long Road to Diagnosis
Imagine waking up every morning with numb hands. Not the “I slept on it wrong” numbness that fades in seconds, but a profound loss of sensation in the hand, wrist, or elbow that takes several minutes to resolve, accompanied by aggressive pins and needles.
For many sufferers, this has been going on for years. They also develop a persistent, dull ache in the wrist and hand, specifically affecting the peripheral (outer) aspect of the hand and forearm. When they seek medical help, the logical assumption is spinal pathology. After all, many patients work in office environments with prolonged sitting or perform repetitive overhead tasks.
The “usual suspects” come to mind: cervical radiculopathy (a pinched nerve in the neck), carpal tunnel syndrome, or perhaps even multiple sclerosis.
As a result, patients undergo extensive testing. They receive an MRI of the brain and cervical spine, which often comes back “normal.” The report may note well-spaced vertebrae, normal discs, normal facet joints, and even a “generous central canal”—the opposite of a narrow spine. X-rays find no cervical ribs (a known cause of TOS, but not the only one). Neurophysiology studies show normal nerve conduction in the median and ulnar nerves, effectively ruling out carpal tunnel syndrome.
Everything points away from the spine. Yet the patient continues to suffer. Some even experience episodes where morning numbness and tingling affect multiple limbs, causing significant distress and functional limitation.
What is Thoracic Outlet Syndrome (TOS)?
To understand why so many patients get stuck in diagnostic limbo, we have to look at anatomy outside the spinal column. The thoracic outlet is the space between your collarbone (clavicle) and your first rib. This narrow passageway is a busy intersection for critical nerves (the brachial plexus) and blood vessels (the subclavian artery and vein).
When this space becomes compressed, you get Thoracic Outlet Syndrome. There are three primary types:
- Neurogenic TOS (most common, affecting the nerves).
- Venous TOS (affecting veins, causing swelling and discolouration).
- Arterial TOS (least common but most dangerous, affecting arteries).
However, there is a vascular component to TOS that is often overlooked. In many cases, the clincher is that the symptoms are not just nerve pain—they are vascular. The compression is affecting blood flow, leading to a distinct set of signs that differ from typical radiculopathy.
The “Aha!” Moment: Two Key Diagnostic Tests
During a thorough clinical examination, healthcare providers can perform two specific provocative tests that often change the entire direction of care: the Roos Test and Adson’s Test.
The Roos Test (also known as the Hands-Up Test) requires the patient to open and close their hands with arms abducted to 90 degrees and externally rotated. In a positive test, the radial pulse diminishes (meaning blood flow is being obstructed), and the patient reproduces their exact symptoms: heaviness, pins and needles in the fingers or wrist, and pain spreading toward the elbow.
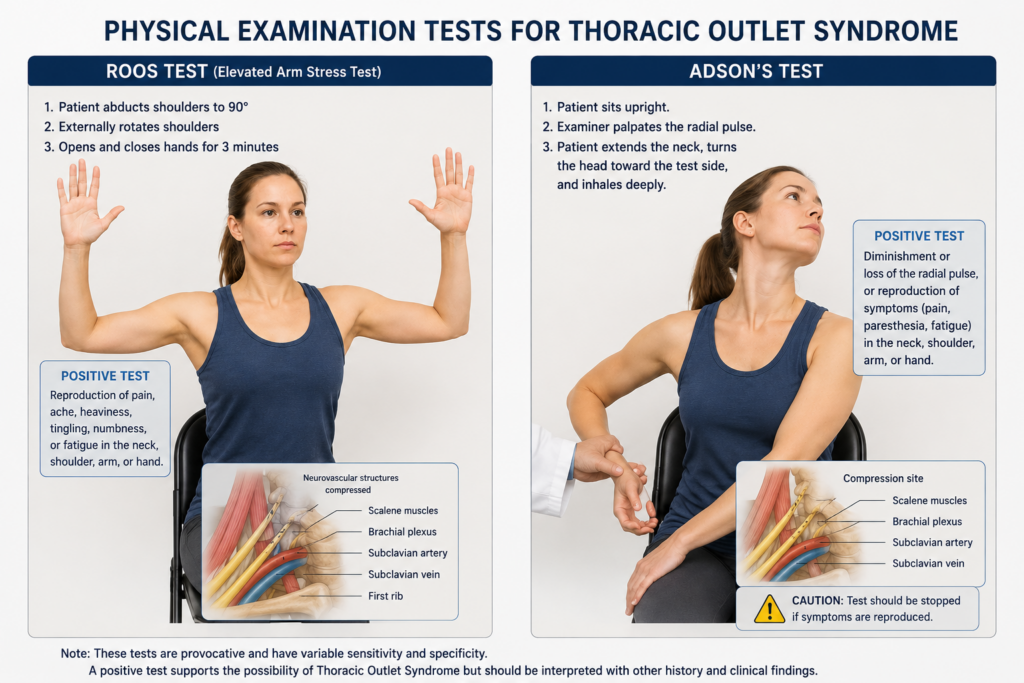
Adson’s Test involves positioning the head and neck while the patient inhales deeply. Again, the clinician notes a loss of radial pulse and reproduction of tingling symptoms.
Why is this significant? Because if the pulse diminishes with specific arm positions, the issue is mechanical compression of the blood vessels (arteries) passing through the thoracic outlet. This is not a slipped disc. This is not carpal tunnel. This is a structural compression issue likely related to individual anatomy—such as a long transverse process (a bony prominence noted on X-ray) or postural muscle tightness (scalene or pectoralis minor muscles) crushing the vessels.
Why This Isn’t a “Neck” Problem
It is crucial to understand why spinal specialists frequently discharge patients with suspected TOS and refer them elsewhere. The absence of specific clinical findings is actually a positive diagnostic clue.
1. No Neurological “Hard Signs”
Despite significant pain, patients with vascular TOS usually have a full cervical range of motion, including rotation, flexion, extension, and lateral flexion. Power is typically preserved (5/5) in the major myotomes. Reflexes (brachioradialis, biceps, triceps) remain normal. Grip strength is strong. If a patient had a true cervical radiculopathy (such as a C6 or C7 nerve root compression), they would likely have weakness in specific muscle groups or diminished reflexes. In TOS, those signs are absent.
2. Negative Compression Testing
When a clinician presses down on the head (cervical compression test), a patient with a disc herniation will usually experience radicular symptoms—pain shooting down the arm. In TOS, the same test only elicits a local pulling sensation in the neck. That effectively rules out a disc herniation irritating a nerve root.
3. The “Morning” Pattern
Spinal pain generally worsens with activity. Vascular TOS often worsens at night or in the morning. Why? Because during sleep, the shoulders tend to droop or fall forward, narrowing the thoracic outlet. The patient woke up with a “dead” arm because blood flow was partially occluded during the night. The several minutes it takes to regain sensation is the time required for blood flow to return once the patient sits up and opens the shoulder girdle.
The Vascular Connection: A Red Flag
One of the most concerning features of vascular TOS is the potential for episodes involving multiple limbs. If the compression is significant enough to occlude the subclavian artery (which supplies the arm), it can sometimes affect related vascular structures, depending on the head and neck position. Bilateral TOS (affecting both sides) can mimic systemic disorders like multiple sclerosis or central cord syndrome.
Patients with vascular TOS often find themselves in a frustrating diagnostic loop. They may be referred to rheumatology (with normal blood tests), neurology (with normal nerve studies), and orthopaedics (with normal spine imaging). All tests come back normal. This is the classic “homeless” patient of the medical world—too complex for the spine surgeon, too vascular for the neurologist.
What Happens Next? The Proper Referral Pathway
When a thorough spinal assessment rules out cervical myelopathy, radiculopathy, and carpal tunnel syndrome—and provocative tests like Roos and Adson’s are positive—the appropriate next step is referral to a vascular specialist.
For the office worker or manual labourer suffering from unexplained upper limb symptoms, the journey changes direction at this point. Here is what the vascular team will typically look for and recommend:
1. Advanced Imaging
Standard X-rays are not enough. The vascular team will likely order an MRA (Magnetic Resonance Angiogram) or a CT angiogram. While plain X-rays may show “no cervical ribs,” they might note a “long transverse process.” This bony prominence can be sharp enough to abrade the subclavian artery. The vascular team needs to assess for the presence of an aneurysm or thrombus in the subclavian artery, which can be a serious complication of untreated vascular TOS.
2. Specialised Physical Therapy
Unlike general neck pain, TOS requires specific stretching of the scalene and pectoralis minor muscles. General cervical strengthening is not enough—the patient needs to strengthen the rhomboids and lower trapezius to open up the thoracic outlet. Ergonomic changes are also critical: adjusting workstations so the patient is not reaching forward, avoiding overhead lifting, and modifying sleep positions.
3. Surgical Intervention
Given positive vascular signs (diminished pulse with arm movement), surgery is a distinct possibility. A vascular surgeon might perform a transaxillary first rib resection—removing the first rib to create space in the thoracic outlet. If a long transverse process or cervical rib variant is present, that may also be excised. Surgical outcomes for vascular TOS are generally excellent when the condition is properly diagnosed.
Lessons for the Chronic Pain Sufferer
If you are reading this and recognise yourself in this description—morning numbness, dull wrist aches, normal spine MRIs, and a feeling that doctors think you are imagining things—consider these takeaways:
- The spine isn’t always the culprit. A normal MRI of the neck is good news. It means your spinal cord is safe. But it also tells you to look elsewhere for the source of your symptoms.
- Check your pulse. If you turn your head to one side, lift your arm, and feel your wrist pulse disappear or your symptoms flare up, you may have vascular TOS. This is a simple screening manoeuvre you can discuss with your doctor.
- Beware the “wastebasket” diagnosis. Carpal tunnel syndrome is over-diagnosed. If your nerve conduction studies are normal, but you have pain in the peripheral aspect of the hand (the ring and little finger side) and elbow pain, think TOS.
- Advocate for the right specialist. If you have ruled out spinal pathology, you likely do not need a spine surgeon or a rheumatologist. You need a vascular surgeon. Do not hesitate to request this specific referral.
Conclusion
Thoracic Outlet Syndrome, particularly the vascular subtype, is a classic example of a condition that requires strong differential diagnosis skills. The symptoms may look like a neck problem, feel like a nerve problem, and present like a systemic disorder. But because the pathology is in the thoracic outlet rather than the cervical spine, the treatment is radically different.
Sufferers do not need spinal fusion. They do not need carpal tunnel release. They need the thoracic outlet decompressed.
Thanks to thorough clinical assessment—including provocative tests like Roos and Adson’s—patients with this condition can finally be placed on the right diagnostic path. For anyone suffering from unexplained neck pain and “dead arms” in the morning, remember: sometimes the problem isn’t in your spine. It is in the tiny, crowded space between your collarbone and your first rib.
Disclaimer: This blog post is based on clinical educational material and is not a substitute for professional medical advice. If you are experiencing similar symptoms, please consult a physician or a vascular specialist for a proper evaluation.