Nerve tension is pain that occurs because a nerve is being compressed or stuck in its surrounding tissue which prevents it from moving within its track like it normally does. This can happen for a variety of reasons.
Physiotherapy plays a crucial role in the treatment of nerve root entrapment by focusing on relieving pain, reducing inflammation, improving mobility, and restoring function. A physiotherapist will typically develop a personalized treatment plan based on the individual’s specific symptoms, underlying condition, and overall health. Here are some common physiotherapy interventions for nerve root entrapment:
Manual Therapy Techniques:
a. Soft Tissue Mobilization: The physiotherapist may use hands-on techniques such as massage, myofascial release, or trigger point therapy to alleviate muscle tension, reduce scar tissue, and improve blood flow in the affected area.
b. Joint Mobilization: Gentle, controlled movements applied to the spine or other affected joints can help restore normal joint function, relieve stiffness, and reduce nerve compression.
c. Spinal Traction: Traction techniques may be employed to create space between vertebrae, decompressing the nerve root and relieving pain.
2. Exercise Therapy:
a. Stretching: Targeted stretching exercises can improve flexibility and relieve tension in the muscles surrounding the affected nerve root.
b. Strengthening: Strengthening exercises focus on supporting muscles to enhance stability and reduce stress on the affected area. The physiotherapist will design a program that targets specific muscle groups to improve posture and core strength.
c. Low-Impact Aerobic Exercise: Activities such as swimming or stationary biking may be recommended to improve cardiovascular fitness without placing excessive strain on the spine.
3. Postural Education and Ergonomics:
a. The physiotherapist may assess the patient’s posture and guide proper body mechanics and ergonomics. This includes recommendations for maintaining good posture during daily activities, such as sitting, standing, lifting, and sleeping.
b. Ergonomic modifications, such as adjusting workstations or using supportive pillows, may be suggested to minimize strain on the spine and nerves.
4. Pain Management Techniques:
a. Heat and Cold Therapy: The application of heat packs or cold packs can help reduce pain and inflammation in the affected area.
b. Transcutaneous Electrical Nerve Stimulation (TENS): TENS units deliver low-level electrical impulses to the affected area, which can help block pain signals and provide temporary pain relief.
c. Ultrasound Therapy: The use of ultrasound waves can promote healing, reduce inflammation, and relieve pain, This treatment is no longer advised for back according to the NICE guidelines for the treatment of back pain.
5. Education and Self-Management Strategies:
a. The physiotherapist will provide education on self-management techniques, such as correct body mechanics, posture, and exercises that can be continued at home.
b. The patient will be guided on activity modification and advised on which activities to avoid or modify to prevent exacerbating symptoms.
It’s important to note that physiotherapy for nerve root entrapment should be conducted under the guidance of a qualified physiotherapist or healthcare professional. They will monitor progress, adjust the treatment plan as needed, and ensure that exercises and techniques are performed safely and effectively.
Nerve root entrapment, also known as radiculopathy, is a condition characterized by the compression or irritation of nerve roots in the spinal column. This condition can cause significant pain, numbness, weakness, and other symptoms along the path of the affected nerve. Treatment for nerve root entrapment aims to relieve the compression on the nerve and manage the associated symptoms. Here are some common treatment approaches:
Non-Surgical Treatments:
a. Rest and Activity Modification: Taking a break from activities that exacerbate the symptoms can help reduce inflammation and allow the nerve to heal.
b. Physical Therapy: Targeted exercises and stretches can improve flexibility, strengthen supportive muscles, and alleviate pressure on the affected nerve.
c. Pain Medications: Over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs) or prescription medications may be recommended to manage pain and reduce inflammation.
d. Hot and Cold Therapy: Applying heat or cold packs to the affected area can help reduce pain and inflammation.
e. Epidural Steroid Injections: In some cases, corticosteroid injections may be administered directly into the space around the affected nerve root to reduce inflammation and alleviate symptoms.
2. Surgical Treatments:
a. Microdiscectomy: This minimally invasive procedure involves removing a portion of the herniated or protruding disc that is compressing the nerve root.
b. Laminectomy: In cases where there is significant spinal stenosis or bone overgrowth causing nerve compression, a laminectomy may be performed to remove the lamina (a portion of the vertebral bone) to create more space for the nerve roots.
c. Foraminotomy: This procedure involves enlarging the opening through which the nerve root exits the spinal canal, providing more room and relieving pressure on the nerve.
The choice of treatment depends on various factors, including the severity of symptoms, the underlying cause of nerve root entrapment, and the individual patient’s overall health. Conservative treatments are typically the first line of approach, with surgery considered if symptoms persist or worsen despite non-surgical interventions.
It is important to consult with a healthcare professional, such as a neurologist, orthopedic surgeon, or spine specialist, who can assess the specific condition and provide appropriate treatment recommendations tailored to the individual’s needs.
In 1981, Palmer and Werner introduced the term triangular fibrocartilage complex (TFCC) to describe the ligamentous and cartilaginous structures that suspend the distal radius and ulnar carpus from the distal ulna (see the image below).[1] The TFCC is the major ligamentous stabiliser of the distal radioulnar (DRU) joint and the ulnar carpus.
The triangular fibrocartilage complex suspends the distal radius and ulnar carpus from the distal ulna. T=triquetrum; L=lunate; S=scaphoid. (Reprinted with permission from Palmer AK and Werner FW: The Triangular Fibrocartilage Complex of the Wrist Anatomy and Function. J Hand Surg; 1981; 6:153)
Functions of the TFCC are as follows:
It provides a continuous gliding surface across the entire distal face of the two forearm bones for flexionextension and translational movements (see the first image below)
It provides a flexible mechanism for stable rotational movements of the radiocarpal unit around the ulnar axis
It suspends the ulnar carpus from the dorsal ulnar face of the radius
It cushions the forces transmitted through the ulnocarpal axis
It solidly connects the ulnar axis to the volar carpus (see the second image below)
The triangular fibrocartilage complex provides a continuous gliding surface across the entire distal face of the radius and ulna to allow for flexionextension and translational movements.
10/11/2015 Triangular Fibrocartilage Complex Injuries: Background, History of the Procedure, Problem
Distally, the triangular fibrocartilage complex inserts into the lunate and triquetrum via the ulna lunate and ulna triquetral ligaments. The triangular fibrocartilage complex solidly connects the ulnar axis to the volar carpus. The unlabeled arrow points to the pre-styloid recess. (Reprinted with permission from Palmer AK and Werner FW: The Triangular Fibrocartilage Complex of the Wrist Anatomy and Function. J Hand Surg; 1981; 6:153)
History of the Procedure
Since 1777, when DeSault’s original dissertation first described DRU joint injuries, much has been written about this joint and the TFCC. As Palmer pointed out,[1, 2, 3] humans are differentiated from lower primates by a radiocarpal joint with a TFCC interposed between the ulna and carpus.[1] This TFCC improves wrist functional stability and allows six degrees of freedom at the wrist—flexion, extension, supination, pronation, and radial and ulnar deviation.
As interest in the TFCC evolved, open repair techniques for this structure were devised. Small joint arthroscopy provides the opportunity for new techniques in the debridement or repair of these structures.
Problem
Injuries to the TFCC present as ulnarside wrist pain, frequently with clicking. Torn TFCCs constitute 35% of intraarticular fractures and 53% of extraarticular fractures. There is no correlation between ulnar styloid fractures and TFCC injuries. Patients with a torn TFCC display ulnar variance (radial shortening) that is on average 4.6 mm (vs 2.5 mm for no tear) and dorsal angulation of 24° (vs 12° for no tear).
Epidemiology Frequency
Mikic looked at 180 wrist joints in 100 cadavers, ranging in age from fetuses to 94 years.[4] He demonstrated that degeneration of the TFCC begins in the third decade of life and progressively increases in frequency and severity in subsequent decades. After the fifth decade of life, he noted no normalappearing TFCCs. Viegas and Ballantyne found similar results.[5]
Etiology
Causative conditions for TFCC injuries include the following:
Falls onto pronated hyperextended wrist
Powerdrill injuries in which the drill binds and rotates the wrist instead of the bit
Distraction force applied to the volar forearm or wrist
Distal radius fractures
Pathophysiology
Palmer and Werner looked at the axial load distribution through the distal radius and ulna[6] and demonstrated that with normal axial loading, 20% of the force is transmitted through the ulna and 80% through the radius. Their data also illustrated that small changes in relative ulnar length can significantly alter load patterns across the wrist. For example, with a distal radius fracture that settles 2.5 mm, an increase in the ulnar axial load of approximately 40% can be expected.
Palmer, Werner, Glisson, and Murphy demonstrated that the percentage of axial force transmitted through the ulna decreases by sequential removal of the horizontal portion of the TFCC.[7] This percentage decrease is accentuated with more positive ulnar variance.
In a cadaver study, Adams demonstrated that no significant kinematic or structural changes resulted from an excision that did not violate the peripheral 2 mm of the disk and that constituted less than two-thirds of the disk area.[8]
TFCC tears are associated with a positive ulnar variance. Ulnar variance increases with pronation and grip and decreases with supination.
The floor of the extensor carpi ulnaris (ECU) tendon sheath broadly connects with the TFCC. After the release of the TFCC from its distal ulna attachment, Tang demonstrated a 30% increase in ECU tendon excursion during wrist extension.[9] This suggests the following:
10/11/2015 Triangular Fibrocartilage Complex Injuries: Background, History of the Procedure, Problem
The TFCC is an important pulley for the ECU tendon
Disruption of the normal ECU excursion may contribute to abnormal loading and force transmission through the ulnar wrist and TFCC
Presentation
The history of TFCC injuries includes ulnarside wrist pain (frequently accompanied by clicking), a fall or trauma, and/or mechanical symptoms that improve with rest and worsen with activity.
In the physical examination, look for the following:
Painful grinding or clicking with wrist range of motion (ROM)
Weakness
Ulnar deviation of the wrist with the forearm in neutral produces ulnar wrist pain and occasional clicking (perform a TFCC compression test)
Instability of the DRU joint with shucking the distal radius and ulna between the examiner’s fingers (perform a DRU joint stress test; always compare this with the opposite wrist)
Piano key sign, which is a prominent and ballottable distal ulna with full pronation of the forearm
Ulnar carpal sag
Lunotriquetral (LT) interval tenderness
Positive LT ballottement or shuck test
ECU tendon subluxation
Indications
If a congruent reduction cannot be achieved or if the dorsal instability is unstable in 30° of supination, then arthroscopic evaluation of the TFCC is recommended with repair as needed.
Relevant Anatomy
As the name suggests, the TFCC is triangular in shape. Palmer found an inverse relation between ulnar variance and TFCC thickness of the TFCC: The TFCC is thicker in individuals who are ulnar minus.[7] Generally, the TFCC is 12 mm thick at its centre. This may thicken to 5 mm where the TFCC inserts into the eccentric concavity of the ulnar head and projecting styloid.
The TFCC extends ulnarly to insert into the base of the ulnar styloid (see the first image below). Distally, it inserts into the lunate via the ulna lunate (UL) ligament and the triquetrum via the ulna triquetral (UT) ligament (see the second image below), hamate, and base of the fifth metacarpal. Radially, the TFCC arises from the ulnar margin of the lunate fossa of the radius (see the third image below).
Relation of the triangular fibrocartilage complex to the distal radius and ulnar styloid.
The ulnocarpal portion of the triangular fibrocartilage complex is composed of the discus articularis, the ulna lunate (ULL), and the ulna triquetral (UTL) ligaments. Distally, the triangular fibrocartilage complex inserts into the lunate via the ulna lunate ligament and into the triquetrum via the ulna triquetral ligament.
10/11/2015 Triangular Fibrocartilage Complex Injuries: Background, History of the Procedure, Problem
Sigmoid notch of the distal radius with distinct dorsal, palmar, and distal margins and an indistinct proximal margin; the triangular fibrocartilage complex arises from the ulnar margin of the lunate fossa of the radius. (Reprinted with permission from Fernandez D and Palmer AK. Fractures of the Distal Radius. In: Green’s Operative Hand Surgery. Vol 1. 1999)
Underneath the TFCC is the ulnar head. The seat, or the convex portion of the ulnar head, articulates with the sigmoid notch of the radius (see the image below). The cartilagecovered nonarticular pole of the ulnar head is deep to the articular disk.
The seat of the ulnar head articulates with the sigmoid notch of the distal radius. Radially, the triangular fibrocartilage complex arises from the ulnar margin of the lunate fossa of the radius. Ulnarly, the triangular fibrocartilage complex inserts into the base of the ulnar styloid. (Reprinted with permission from Fernandez D and Palmer AK. Fractures of the Distal Radius. In: Green’s Operative Hand Surgery. Vol 1. 1999)
The ulnocarpal portion of the TFCC is composed of the discus articularis and the UL and UT ligaments (referred to by some as the disk carpal ligaments). Embryologic studies have demonstrated that these ligaments arise from the disk and are critical to the carpal suspensory function of the TFCC.
The dorsal and palmar branches of the anterior interosseous artery and dorsal and palmar radiocarpal branches from the ulnar artery supply blood to the periphery of the TFCC. These vessels supply the TFCC in a radial fashion, with histologic sections demonstrating that the vessels penetrate the peripheral 1040% of the disk. The central portion and radial attachment are avascular.
Mikic demonstrated that the percentage of the peripheral disk that is vascularized is reduced by one-third in a young patient to one fourth in patients of advanced age. [4]
Because the periphery of the TFCC has a good blood supply, tears in this region can be repaired. By contrast, tears in the central avascular area must be debrided because they have no potential for healing.
The richly vascularized DRU ligament and palmar radioulnar (PRU) ligament are composed of thick, longitudinally oriented collagen fibre bundles that blend in with the central avascular fibrocartilaginous portion.
When the TFCC is viewed during wrist arthroscopy, the styloid attachment appears folded. Some of the blood vessels to the TFCC enter between these folds. This fold, combined with the vascular hilum, is termed the ligamentum subcruentum, which actually is the confluence of the TFCC and the Vshaped ligament (disk ligament) as it extends from the hilar area of the styloid to its twin insertions on the lunate and triquetrum.
From a distal perspective, the TFCC has two distinct insertions into the ulna—a superficial portion and a deep portion. The superficial components, the DRU and PRU ligaments, insert into the base of the styloid. The deep portion, the ligamentum subcruentum, inserts into the fovea near the axis of forearm rotation.
Contraindications
Repairing TFCC tears is contraindicated in the presence of infection or
10/11/2015 Triangular Fibrocartilage Complex Injuries: Background, History of the Procedure, Problem
degeneration. Palmer class 2 degenerative TFCC tears (see the Palmer classification for TFCC abnormalities in Medical therapy) represent a pathologic progression of disease associated with ulnar impaction syndrome.
Degeneration of the TFCC is found with repetitive pronation and axial grip loading in association with ulnar positive variance and impaction between the ulnar head and the proximal pole of the lunate. Treatment of degenerative TFCC tears associated with ulnar impaction syndrome consists of nonoperative treatment first with immobilisation, avoidance of aggravating activities, and nonsteroidal anti inflammatory drugs (NSAIDs).
Palmer class 2A and 2B lesions that fail to respond to conservative treatment are treated with gentle debridement. If the patient is ulnar positive and symptomatic, a formal ulnar shortening is considered. An arthroscopic wafer is contraindicated, as this would require resection of intact TFCC to perform the procedure or require performing the procedure entirely through the DRU joint portals.
The surgical indications for an arthroscopic wafer procedure are a Palmer class 2C or 2D lesion in an ulnar positive variance of not more than 2 mm without evidence of lunatetriquetrum instability. If lunatetriquetrum instability is present, this is addressed with formal ulnar shortening in an attempt to tighten the ulnocarpal ligaments and decrease the motion between the lunate and triquetrum.
For patients with an ulnar positive variance of more than 2 mm, formal ulnar shortening is performed. For patients with ulnar neutral or negative variance and a Palmer class 2C lesion, an arthroscopic debridement is performed. Palmer class 2E lesions respond unpredictably to arthroscopic debridement. They are usually treated with a salvage procedure such as a limited ulnar head resection, SauveKapandji procedure, or Darrach procedure that addresses the DRU joint and LT joint pathology.
Workup
Contributor Information and Disclosures
Author
James R Verheyden, MD Consulting Surgeon, Department of Orthopedic Surgery, The Orthopedic and Neurosurgical Center of the Cascades
James R Verheyden, MD is a member of the following medical societies: American Academy of Orthopaedic Surgeons, American Medical Association, American Society for Surgery of the Hand
Disclosure: Nothing to disclose.
Coauthor(s)
Andrew K Palmer, MD Chair, Professor, Department of Orthopedics, State University of New YorkUpstate Medical University
Andrew K Palmer, MD is a member of the following medical societies: American Osteopathic College of Physical Medicine and Rehabilitation
Disclosure: Partner received salary from Del Palma Orthopedics for board membership.
Specialty Editor Board
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; EditorinChief, Medscape Drug Reference
Disclosure: Received salary from Medscape for employment. for: Medscape.
N Ake Nystrom, MD, PhD Associate Professor of Orthopedic Surgery and Plastic Surgery, University of Nebraska Medical Center
Disclosure: Nothing to disclose.
Chief Editor
Harris Gellman, MD Consulting Surgeon, Broward Hand Center; Voluntary Clinical Professor of Orthopedic Surgery and Plastic Surgery, Departments of Orthopedic Surgery and Surgery, University of Miami, Leonard M Miller School of Medicine, Clinical Professor, Surgery, Nova Southeastern School of Medicine
Harris Gellman, MD is a member of the following medical societies: American Academy of Medical Acupuncture, American Academy of Orthopaedic Surgeons, American Orthopaedic Association, American Society for Surgery of the Hand, Arkansas Medical Society
Disclosure: Nothing to disclose.
Additional Contributors
Joseph E Sheppard, MD Professor of Clinical Orthopedic Surgery, Chief of Hand and Upper Extremity Service, Department of Orthopedic Surgery, University of Arizona Health Sciences Center, University Physicians Healthcare
Joseph E Sheppard, MD is a member of the following medical societies: American Academy of Orthopaedic Surgeons, Orthopaedics Overseas, American Society for Surgery of the Hand
Disclosure: Nothing to disclose.
References
Palmer AK, Werner FW. The triangular fibrocartilage complex of the wristanatomy and function. J Hand Surg [Am]. 1981 Mar. 6(2):15362. [Medline].
Palmer AK. Triangular fibrocartilage complex lesions: a classification. J Hand Surg [Am]. 1989 Jul. 14(4):594606. [Medline].
Palmer AK, Glisson RR, Werner FW. The relationship between ulnar variance and triangular fibrocartilage complex thickness. J Hand Surg [Am]. 1984 Sep. 9(5):6812. [Medline].
10/11/2015 Triangular Fibrocartilage Complex Injuries: Background, History of the Procedure, Problem
Mikic ZD. Age changes in the triangular fibrocartilage of the wrist joint. J Anat. 1978 Jun. 126(Pt 2):36784. [Medline].
Viegas SF, Ballantyne G. Attritional lesions of the wrist joint. J Hand Surg [Am]. 1987 Nov. 12(6):10259. [Medline].
Palmer AK, Werner FW. Biomechanics of the distal radioulnar joint. Clin Orthop Relat Res. 1984 JulAug. 2635. [Medline].
Palmer AK, Werner FW, Glisson RR, Murphy DJ. Partial excision of the triangular fibrocartilage complex. J Hand Surg [Am]. 1988 May. 13(3):3914. [Medline].
Adams BD. Partial excision of the triangular fibrocartilage complex articular disk: a biomechanical study. J Hand Surg [Am]. 1993 Mar. 18(2):33440. [Medline].
Tang JB, Ryu J, Kish V. The triangular fibrocartilage complex: an important component of the pulley for the ulnar wrist extensor. J Hand Surg [Am]. 1998 Nov. 23(6):98691. [Medline].
Yoshioka H, Tanaka T, Ueno T, Carrino JA, Winalski CS, Aliabadi P, et al. Study of ulnar variance with high resolution MRI: correlation with triangular fibrocartilage complex and cartilage of ulnar side of wrist. J Magn Reson Imaging. 2007 Sep. 26(3):7149. [Medline].
Zlatkin MB, Rosner J. MR imaging of ligaments and triangular fibrocartilage complex of the wrist. Radiol Clin North Am. 2006 Jul. 44(4):595623, ix. [Medline].
Iordache SD, Rowan R, Garvin GJ, Osman S, Grewal R, Faber KJ. Prevalence of triangular fibrocartilage complex abnormalities on MRI scans of asymptomatic wrists. J Hand Surg Am. 2012 Jan. 37(1):98103. [Medline].
Richards RS, Bennett JD, Roth JH, Milne K Jr. Arthroscopic diagnosis of intraarticular soft tissue injuries associated with distal radial fractures. J Hand Surg [Am]. 1997 Sep. 22(5):7726. [Medline].
Lee Master D, Yao J. The wrist insufflation test: a confirmatory test for detecting intercarpal ligament and triangular fibrocartilage complex tears. Arthroscopy. 2014 Apr. 30(4):4515. [Medline].
Osterman AL, Terrill RG. Arthroscopic treatment of TFCC lesions. Hand Clin. 1991 May. 7(2):27781. [Medline].
Rettig ME, Raskin KB. Galeazzi fracturedislocation: a new treatmentoriented classification. J Hand Surg [Am]. 2001 Mar. 26(2):22835. [Medline].
Geel CW, Palmer AK. Radial head fractures and their effect on the distal radioulnar joint. A rationale for treatment. Clin Orthop Relat Res. 1992 Feb. 7984. [Medline].
McAdams TR, Swan J, Yao J. Arthroscopic Treatment of Triangular Fibrocartilage Wrist Injuries in the Athlete. Am J Sports Med. 2008 Dec 4. [Medline].
Yao J, Dantuluri P, Osterman AL. A novel technique of allinside arthroscopic triangular fibrocartilage complex repair. Arthroscopy. 2007 Dec. 23(12):1357.e14. [Medline].
Yao J. Allarthroscopic triangular fibrocartilage complex repair: safety and biomechanical comparison with a traditional outsidein technique in cadavers. J Hand Surg [Am]. 2009 Apr. 34(4):6716. [Medline].
Anderson ML, Larson AN, Moran SL, Cooney WP, Amrami KK, Berger RA. Clinical comparison of arthroscopic versus open repair of triangular fibrocartilage complex tears. J Hand Surg [Am]. 2008 MayJun. 33(5):67582. [Medline].
Reiter A, Wolf MB, Schmid U, Frigge A, Dreyhaupt J, Hahn P, et al. Arthroscopic repair of Palmer 1B triangular fibrocartilage complex tears. Arthroscopy. 2008 Nov. 24(11):124450. [Medline].
Varitimidis SE, Basdekis GK, Dailiana ZH, Hantes ME, Bargiotas K, Malizos K. Treatment of intraarticular fractures of the distal radius: fluoroscopic or arthroscopic reduction?. J Bone Joint Surg Br. 2008 Jun. 90(6):77885. [Medline].
Wysocki RW, Richard MJ, Crowe MM, Leversedge FJ, Ruch DS. Arthroscopic Treatment of Peripheral Triangular Fibrocartilage Complex Tears With the Deep Fibers Intact. J Hand Surg Am. 2012 Feb 1. [Medline].
Chen AC, Hsu KY, Chang CH, Chan YS. Arthroscopic suture repair of peripheral tears of triangular fibrocartilage complex using a volar portal. Arthroscopy. 2005 Nov. 21(11):1406. [Medline].
Wnorowski DC, Palmer AK, Werner FW, Fortino MD. Anatomic and biomechanical analysis of the arthroscopic wafer procedure. Arthroscopy. 1992. 8(2):20412. [Medline].
Henry MH. Management of acute triangular fibrocartilage complex injury of the wrist. J Am Acad Orthop Surg. 2008 Jun. 16(6):3209. [Medline].
de Araujo W, Poehling GG, Kuzma GR. New Tuohy needle technique for triangular fibrocartilage complex repair: preliminary studies. Arthroscopy. 1996 Dec. 12(6):699703. [Medline].
Sagerman SD, Short W. Arthroscopic repair of radialsided triangular fibrocartilage complex tears. Arthroscopy. 1996 Jun. 12(3):33942. [Medline].
Trumble TE, Gilbert M, Vedder N. Isolated tears of the triangular fibrocartilage: management by early arthroscopic repair. J Hand Surg [Am]. 1997 Jan. 22(1):5765. [Medline].
Corso SJ, Savoie FH, Geissler WB, et al. Arthroscopic repair of peripheral avulsions of the triangular fibrocartilage complex of the wrist: a multicenter study. Arthroscopy. 1997 Feb. 13(1):7884. [Medline].
Lucey SD, Poehling GG. Arthroscopic treatment of triangular fibrocartilage complex tears. In: Techniques in Hand and Upper Extremity Surgery. Vol 1. Philadelphia, Pa: Lippincott Williams & Wilkins;. 1997: 22836.
Nakamura T, Yabe Y, Horiuchi Y. Fat suppression magnetic resonance imaging of the triangular fibrocartilage complex. Comparison with spin echo, gradient echo pulse sequences and histology. J Hand Surg [Br]. 1999 Feb. 24(1):226. [Medline].
Skie MC, Mekhail AO, Deitrich DR, Ebraheim NE. Operative technique for insideout repair of the triangular fibrocartilage complex. J Hand Surg [Am]. 1997 Sep. 22(5):8147. [Medline].
10/11/2015 Triangular Fibrocartilage Complex Injuries: Background, History of the Procedure, Problem
Desai MJ, Hutton WC, Jarrett CD. Arthroscopic repair of triangular fibrocartilage tears: a biomechanical comparison of a knotless suture anchor and the traditional outsidein repairs. J Hand Surg Am. 2013 Nov. 38(11):21937. [Medline].
Minami A, Ishikawa J, Suenaga N, Kasashima T. Clinical results of treatment of triangular fibrocartilage complex tears by arthroscopic debridement. J Hand Surg [Am]. 1996 May. 21(3):40611. [Medline].
Westkaemper JG, Mitsionis G, Giannakopoulos PN, Sotereanos DG. Wrist arthroscopy for the treatment of ligament and triangular fibrocartilage complex injuries. Arthroscopy. 1998 JulAug. 14(5):47983. [Medline].
De Smet L, Van Nuffel M, Koorneef P, Degreef I. Arthroscopic debridement with and without distal ulnar resection in the treatment of triangular fibrocartilage complex tears. Acta Orthop Belg. 2014 Mar. 80(1):112 5. [Medline].
Minami A, Kato H. Ulnar shortening for triangular fibrocartilage complex tears associated with ulnar positive variance. J Hand Surg [Am]. 1998 Sep. 23(5):9048. [Medline].
Trumble TE, Gilbert M, Vedder N. Ulnar shortening combined with arthroscopic repairs in the delayed management of triangular fibrocartilage complex tears. J Hand Surg [Am]. 1997 Sep. 22(5):80713. [Medline].
Hulsizer D, Weiss AP, Akelman E. Ulnashortening osteotomy after failed arthroscopic debridement of the triangular fibrocartilage complex. J Hand Surg [Am]. 1997 Jul. 22(4):6948. [Medline].
Yamanaka Y, Nakamura T, Sato K, Toyama Y. How does ulnar shortening osteotomy influence morphologic changes in the triangular fibrocartilage complex?. Clin Orthop Relat Res. 2014 Nov. 472(11):348994. [Medline]. [Full Text].
Nakamura T, Nakao Y, Ikegami H, et al. Open repair of the ulnar disruption of the triangular fibrocartilage complex with double threedimensional mattress suturing technique. Tech Hand Up Extrem Surg. 2004 Jun. 8(2):11623. [Medline].
BaehserGriffith P, Bednar JM, Osterman AL, Culp R. Arthroscopic repairs of triangular fibrocartilage complex tears. AORN J. 1997 Jul. 66(1):1012, 10511, quiz 112, 115, 1178. [Medline].
Bednar JM. Arthroscopic treatment of triangular fibrocartilage tears. Hand Clin. 1999 Aug. 15(3):47988, ix. [Medline].
Bowers WH. The distal radioulnar joint. In: Green’s Operative Hand Surgery. Vol 1. New York, NY: Churchill Livingstone;. 1999: 98995.
Cantor RM, Stern PJ, Wyrick JD, Michaels SE. The relevance of ligament tears or perforations in the diagnosis of wrist pain: an arthrographic study. J Hand Surg [Am]. 1994 Nov. 19(6):94553. [Medline].
Chidgey LK, Dell PC, Bittar ES, Spanier SS. Histologic anatomy of the triangular fibrocartilage. J Hand Surg [Am]. 1991 Nov. 16(6):1084100. [Medline].
Cooney WP. Evaluation of chronic wrist pain by arthrography, arthroscopy, and arthrotomy. J Hand Surg [Am]. 1993 Sep. 18(5):81522. [Medline].
De Smet L, De Ferm A, Steenwerckx A, et al. Arthroscopic treatment of triangular fibrocartilage complex lesions of the wrist. Acta Orthop Belg. 1996 Mar. 62(1):813. [Medline].
Fellinger M, Peicha G, Seibert FJ, Grechenig W. Radial avulsion of the triangular fibrocartilage complex in acute wrist trauma: a new technique for arthroscopic repair. Arthroscopy. 1997 Jun. 13(3):3704. [Medline].
Fernandez DL, Palmer AK. Fractures of the distal radius. In: Green’s Operative Hand Surgery. Vol 1. New York, NY: Churchill Livingstone;. 1999: 9303.
Ishii S, Palmer AK, Werner FW, et al. Pressure distribution in the distal radioulnar joint. J Hand Surg [Am]. 1998 Sep. 23(5):90913. [Medline].
Jantea CL, Baltzer A, Ruther W. Arthroscopic repair of radialsided lesions of the triangular fibrocartilage complex. Hand Clin. 1995 Feb. 11(1):316. [Medline].
Kihara H, Short WH, Werner FW, et al. The stabilising mechanism of the distal radioulnar joint during pronation and supination. J Hand Surg [Am]. 1995 Nov. 20(6):9306. [Medline].
Kirschenbaum D, Sieler S, Solonick D, et al. Arthrography of the wrist. Assessment of the integrity of the ligaments in young asymptomatic adults. J Bone Joint Surg Am. 1995 Aug. 77(8):12079. [Medline].
Kleinman WB, Graham TJ. The distal radioulnar joint capsule: clinical anatomy and role in post-traumatic limitation of forearm rotation. J Hand Surg [Am]. 1998 Jul. 23(4):58899. [Medline].
Nakamura T, Yabe Y, Horiuchi Y. Dynamic changes in the shape of the triangular fibrocartilage complex during rotation demonstrated with high-resolution magnetic resonance imaging. J Hand Surg [Br]. 1999 Jun. 24(3):33841. [Medline].
Nakamura T, Yabe Y, Horiuchi Y. Functional anatomy of the triangular fibrocartilage complex. J Hand Surg [Br]. 1996 Oct. 21(5):5816. [Medline].
Osterman AL. Wrist arthroscopy: Operative procedures. In: Green’s Operative Hand Surgery. Vol 1. New York, NY: Churchill Livingstone;. 1999: 20916.
Schers TJ, van Heusden HA. Evaluation of chronic wrist pain. Arthroscopy superior to arthrography: a comparison in 39 patients. Acta Orthop Scand. 1995 Dec. 66(6):5402. [Medline].
Werner FW, Palmer AK, Fortino MD, Short WH. Force transmission through the distal ulna: effect of ulnar variance, lunate fossa angulation, and radial and palmar tilt of the distal radius. J Hand Surg [Am]. 1992 May. 17(3):4238. [Medline].
The biceps muscle, one of the muscles in the front of the upper arm bone (or humerus), has two muscle bellies, or heads, that have distinct attachments at the shoulder. These attachments are located at the “proximal” end of the humerus. At the other end of the muscle, near the elbow, the two heads of the biceps join together to form a single distal biceps tendon.
This tendon, located at the “distal” end of the humerus, inserts into the radius bone, one of two bones in the forearm. Through this distal attachment on the radius, the biceps participates in both elbow flexion and supination. Supination is the act of turning the forearm from a “palm down” position to a “palm up” position, such as when tightening a screw with a screwdriver.
Distal Biceps Injury & Symptoms
Injuries to the distal biceps tendon can be partial or complete ruptures. They commonly occur in the dominant arm of middle aged adults. Unanticipated loading of the tendon is a common mechanism of injury when the biceps muscle is contracting but the elbow is rapidly straightened, such as when a heavy object is attempted to be caught when it unexpectantly falls from a height. Typically, the injured tendon has some level of preexisting disease or degeneration, called tendinosis, that makes it vulnerable to injury. Persons who smoke and those who are not physically active are more likely to rupture their biceps tendon when it is subjected to heavy loads.
Presenting symptoms of a distal biceps rupture include pain at the front of the elbow. Sometimes, people with the injury report hearing a “pop” from the area. Pain typically subsides after the acute injury, and if left untreated, a chronic distal biceps rupture is usually not painful. There may be bruising of the skin in association with the injury. If completely ruptured, the tendon can retract toward the shoulder. If this occurs, a cosmetic deformity may be noticeable that looks like a rounded mass in the lower biceps muscle. There may also be a hollow area at the elbow where the tendon used to attach. Most commonly, however, there is not much noticeable change in the appearance of the arm.
From a functional standpoint, some weakness will result in both flexion and supination, or rotation of the forearm. Supination is usually affected more than elbow flexion. However, multiple muscle groups are used in both motions, and no deficit in the functional range of motion will result. The other muscle groups can strengthen to help compensate for the non-functioning, injured biceps. Some residual weakness will be noted, however, for heavy lifting or use a screwdriver, for example.
The diagnosis of a distal biceps rupture can usually be made on patient history and clinical examination. If there is a question of a partial tendon injury or concern of another associated injury (fracture, ligament injury, etc) magnetic resonance imaging (MRI) may be obtained.
How are Distal Biceps Ruptures Treated?
There are several options available for the treatment of a torn distal biceps tendon, ranging from conservative treatment to operative interventions. Most patients will have surgery, but there is a role for nonoperative treatment in the low-demand person or a patient who is a poor surgical candidate. The treating orthopaedic surgeon will discuss these options and help decide the ideal treatment based on patient demands, physical examination, and the type of tear seen on imaging studies including routine x-ray and magnetic resonance imaging (MRI).
A non-operative, physical therapy treatment program will often focus first on reducing pain and maintaining the full motion of the elbow. Oral non-steroidal anti-inflammatory medications (i.e., Ibuprofen) may also be prescribed. After the initial injury, after pain has decreased and the elbow motion is good, treatment may move to muscle strengthening of the other muscles located about the elbow. Painless function with some residual weakness and early fatigue of supination can be achieved through conservative management.
Surgical management focuses on restoring the distal biceps tendon anatomy by repairing the tendon at its insertion site on the radius and allowing it to heal. Surgery is typically performed through an open incision in the front of the elbow or through a two-incision approach, with a small incision in both the front and the back of the elbow.
Chronic ruptures are much more difficult to treat surgically, and sometimes grafts need to be used in this setting. For acute ruptures, the tendon can be reattached to the bone through a variety techniques including sutures, surgical buttons, anchoring devices, and surgical screws.
Rehabilitation
After surgery, the elbow is typically immobilised for a few weeks and then a gentle range of motion exercises are initiated. The majority of tendon healing is usually complete after two months, at which time light strengthening exercises can begin. Return to full activity is variable, but most patients can expect to be back to their pre operative activities by 4-5 months.
‘Shin splints’ or ‘shin splints’ is the common name for what is officially known as for medial tibial stress syndrome.
Pain commonly occurs anywhere along the shinbone from the knee to the ankle. The more common areas for pain are:
on the inner side of the shinbone – ‘medial shin splints’
on the outer side (front of the lower leg) – ‘anterior shin splints’
on both sides of the shin bone in severe cases.
It is a common injury for a wide range of sports such as basketball, soccer and the various football codes. It is also a common running injury, particularly when running on roads and other hard surfaces.
Surprisingly the exact cause of the pain is unknown and may vary among patients. It appears to be caused by strain or over stretching of the muscles and tendons that run along the length of the shin bone causing inflammation. Some recent research suggests it may be a stress reaction in the bone itself, or the muscle attachments to the bone.
The injury appears to be a reaction to the stress of over-exertion or the pounding and jarring associated with many sports. It often occurs in runners which switch their brands of shoes but can occur in barefoot running as well.
Treatment For Shin Splints?
Like most sports injuries treatment includes the regular use of ice packs on the affected area, rest, anti-inflammatory medication such as aspirin and gentle stretching after a few days.
Unfortunately, once they occur it is more likely to happen again. It is worth while looking at what may have triggered the damage. Did you change the shoes you wear or your training routine? Many people find that switching training shoes and adding high quality cushioning insoles lowers the risk of developing shins splints. Increasing training distances slowly and training mostly on grass or other softer surfaces also help. Try to avoid jarring such as occurs when running down hills especially on asphalt. Most people recover within one or two months, without recurrences.
The pain of shin splints is usually mild and it pays to keep active by walking until the pain subsides. Always ramp up the length and intensity of your training slowly. If the pain is severe or prolonged you should see a doctor check for a stress fracture or other more serious injuries.
Stretches for Relief of Shin Splint Pain
A good basic exercise for relief is simple stretching
Stretch 1
Sit in a chair with your sore leg stretched out:
Reach down to grab your toes
Gently pull your toes and foot back toward your body.
Keep stretching for 30-45 seconds
repeat five or six times
reverse the pressure while still holding your toes by gently pushing down for 30-45 seconds
repeat the pushes five or six times.
you can also use an exercise band or cord positioned around the ball of your foot
Stretch 2
Sit on the floor with your feet pressed flat against a wall.
Keep your heels on the ground and knees straight.
With the palms of your hands flat against the floor, lean into the wall and stretch your calf and shin muscles.
Exercise 3
Calf raises help build strength in the muscles at the back of the lower leg, which help support the shin and prevent injuries.
Stand on a flat floor with your feet about six inches (15 cm) apart.
Shift your weight forward from your heels to the balls of your feet.
Rise up on your toes and hold for 30-45 seconds
Roll back and return your heels to the floor
Repeat this exercise 10-15 times
Exercise 4
This exercise is designed to strengthen the tibialis anterior, which is the large muscle on the front lateral side of your shin that is often associated with shin splint injuries.
Sit on the floor with your legs straight out in front, and toes pointing up.
Move your toes toward your body, hold for 10-20 seconds and then slowly release.
Repeat for 10 – 12 repetitions on each side
Advice On Choosing Athletic Sole Insert
Make sure you have a good quality athletic shoe designed for the type of activity that you undertake. Wearing shoes with poorly designed insoles that do not provide adequate cushioning can increase the risks of shin splints. The insoles wear-out and you should consider adding good quality replaceable insoles if you feel comfortable with them. Runners and walkers should replace their shoes regularly.
Stay off the Cement, Bitumen and other Hard Surfaces
Try to train on softer surfaces such as grass, running tracks and crushed gravel. Asphalt is more forgiving than concrete, but timber surfaces are also very hard unless they are suspended or cushioned. However, if you train on grass, be careful the avoid the trap of injuries caused by racing on roads without the right shoes or preparation. One way to reduce the risk of shin splints is to do cross-training. If you’re a runner, add some swimming, cycling, or other exercises that don’t put a strain on your shins. Running up and down hills, especially on roads and hard surfaces may increase the risk of shin splints.
Customized physical therapy may be a useful way to ease low back pain, which affects an estimated 31 million Americans a new study says. Researchers from La Trobe University observed that ‘many patients with low-back disorders persisting beyond 6 weeks do not recover.
Physical therapists do a lot more than just stretch or strengthen weak muscles after an injury or surgery. They are skilled at evaluating and diagnosing potential problems before they lead to more-serious injuries or disabling conditions from carpal tunnel syndrome or a frozen shoulder to chronic headaches or lower back
Let’s talk about 3 tips to get rid of lower back pain from squats. In most cases, pain from squatting comes to technical errors; whether the pain is in the lower back or in the knees. Sometimes, the lower back pain can actually originate from the hips
Remaining in a seated position for extended periods of time can restrict blood flow to your lower extremities, causing flexion, which is a compressive force in the spine. Stopping to stand and stretch is critical for your spine, as it releases the compression, allows for blood to flow to the nerves, and helps maintain flexibility


 Physiotherapy plays a crucial role in the treatment of nerve root entrapment by focusing on relieving pain, reducing inflammation, improving mobility, and restoring function. A physiotherapist will typically develop a personalized treatment plan based on the individual’s specific symptoms, underlying condition, and overall health. Here are some common physiotherapy interventions for nerve root entrapment:
Physiotherapy plays a crucial role in the treatment of nerve root entrapment by focusing on relieving pain, reducing inflammation, improving mobility, and restoring function. A physiotherapist will typically develop a personalized treatment plan based on the individual’s specific symptoms, underlying condition, and overall health. Here are some common physiotherapy interventions for nerve root entrapment:
 Nerve root entrapment, also known as radiculopathy, is a condition characterized by the compression or irritation of nerve roots in the spinal column. This condition can cause significant pain, numbness, weakness, and other symptoms along the path of the affected nerve. Treatment for nerve root entrapment aims to relieve the compression on the nerve and manage the associated symptoms. Here are some common treatment approaches:
Nerve root entrapment, also known as radiculopathy, is a condition characterized by the compression or irritation of nerve roots in the spinal column. This condition can cause significant pain, numbness, weakness, and other symptoms along the path of the affected nerve. Treatment for nerve root entrapment aims to relieve the compression on the nerve and manage the associated symptoms. Here are some common treatment approaches: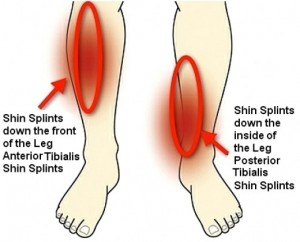
 Surprisingly the exact cause of the pain is unknown and may vary among patients. It appears to be caused by strain or over stretching of the muscles and tendons that run along the length of the shin bone causing inflammation. Some recent research suggests it may be a stress reaction in the bone itself, or the muscle attachments to the bone.
Surprisingly the exact cause of the pain is unknown and may vary among patients. It appears to be caused by strain or over stretching of the muscles and tendons that run along the length of the shin bone causing inflammation. Some recent research suggests it may be a stress reaction in the bone itself, or the muscle attachments to the bone. Stretch 1
Stretch 1